JISRF Activities July 2010
This publication is highlighting
July 21, 2010
 A Flying Commitment to Continuing Education A Flying Commitment to Continuing Education
As a follow up to our recent July 7, 2010 ENews-Update I thought the following story would be a good example of our commitment to CE. It certainly was an educational process for us.
JISRF supports educational activities and some are sponsored by commercial interest. On July 10, 2010 Omnilife scienceTM sponsored a cadaver workshop on their new Apex ARCTM Total Hip Stem and a couple of our TSITM Study Group Members (Charles Bryant, MD., Oklahoma City, OK and Lou Keppler, MD from Cleveland, Ohio) were invited as faculty. The workshop was being held at the Foundation for Orthopaedic Research and Education (foreTM) in Tampa Fl.
 |
If you have not had the opportunity to visit or attend one of their meetings please put it on your "to-do list." Their CEO Dereck Pupello, MBA, has helped make foreTM into a first class research foundation. |
 Dr. Keppler, who is an old friend, and one of my Board members decides he will fly his plane (a twin Areostar) down to the workshop. Ryan (my son) and I decided to keep him company. Our plan was to depart Cleveland after Lou is finished with office hours and make the 800 mile flight down to Tampa Friday night. Then do the cadaver work shop Saturday morning and head back early that afternoon. Just another full weekend. Dr. Keppler, who is an old friend, and one of my Board members decides he will fly his plane (a twin Areostar) down to the workshop. Ryan (my son) and I decided to keep him company. Our plan was to depart Cleveland after Lou is finished with office hours and make the 800 mile flight down to Tampa Friday night. Then do the cadaver work shop Saturday morning and head back early that afternoon. Just another full weekend.
 Now Lou and I go back to the mid 1980’s when he joined Art Steffee’s practice and they both starting doing some S-Rom® stems for me. Lou, in fact, made the first S-Rom surgical video. Together with Hugh Cameron we reported on the seventeen year results at the 2006 AAOS meeting with a scientific exhibit "The Role of Modularity in Primary THA - Is There One?." Needless to say, Lou and I know each other very well. I have flown with Lou a number of times over the years and he is (in his mind) a master pilot. Now I know a little about joint surgery and Lou is the best of the best, but I know nothing about flying except to buckle up. So I take him at his word on his piloting skill set. Now Lou and I go back to the mid 1980’s when he joined Art Steffee’s practice and they both starting doing some S-Rom® stems for me. Lou, in fact, made the first S-Rom surgical video. Together with Hugh Cameron we reported on the seventeen year results at the 2006 AAOS meeting with a scientific exhibit "The Role of Modularity in Primary THA - Is There One?." Needless to say, Lou and I know each other very well. I have flown with Lou a number of times over the years and he is (in his mind) a master pilot. Now I know a little about joint surgery and Lou is the best of the best, but I know nothing about flying except to buckle up. So I take him at his word on his piloting skill set.
 Click here to download PDF Click here to download PDF
|
 S-ROM Hip Course S-ROM Hip Course |
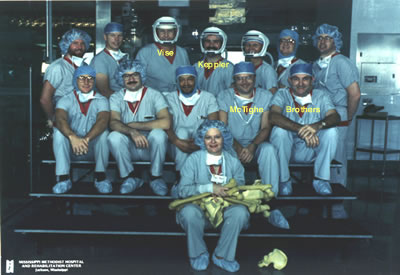
Dr. Keppler and I both have had a long-term commitment to continuing education as depicted by this photo of an S-Rom course held in 1989 and hosted by Dr. Guy Vise in Jackson, Mississippi. Lou was the leading expert on S-Rom® for this course and was doing live surgery in an O.R. setting that could, and did, accommodate all of us. These were exciting and fun times.
Dr. Vise, a wonderful surgeon and friend, as well as John Brothers from Nashville, Tennessee, another good friend, are unfortunately no longer with us. |
However, I digress. Back to my narrative on our trip down to Tampa. So Ryan and I meet up with Lou at the Lorain Country airport west of Cleveland at about 4:30 PM - just after all the mechanics have gone home.
We load up the plane with our overnight bags and instruments for the workshop. Little did we know we would be opening up the ARCTM instrument set before the workshop.
 |
We all get on board, planning on reaching Thomasville, GA about 7:30 PM to pick up Brad Walter, MD, another of our TSITM Study Group members.
Well, Lou is doing his flight check and starts the left engine, however the right engine won’t turn over (start in my language). As all good master surgeons Lou starts talking to himself. Next we are all out of the plane and Lou and Ryan are taking the plane apart. Maybe a little over exaggerated, maybe not. |
The engine is now exposed and a diagnosis is being conducted. The on-site opinion by the master pilot is “the stater is good, but the Bendix is not engaging.” Of course no problem, just free up a little corrosion and we are good to go.
Corrosion - my mind flashes back to John Collier, PhD and how metal corrosion leads to fretting wear and fatigue failure. Am I worried? No. I do as I have my entire career - support my surgeon. After some banging of tools on the engine Lou says let's put it back together and start the engine.
This little plan of action goes on for an hour putting things back together and taking them apart about 3-4 times.
What does a surgeon do when he needs a little help? First try a bigger hammer, then call in a consultation. |
 |
 |
You can see in this photo a ball-peen hammer in his left hand and his cell phone in his right. Still, not to worry.
"We just had the wrong tool. Where is my curved curette?" |
| Notice the sky in the background. We are two hours into this process and a front is moving in while daylight is moving out. "No problem, I just need to spray some silicone to loosen things up." |
 |
 |
Some photos are not being published on account of our friendship.
Parts have now been put on and taken off so many times that I'm now helping with the screwing and unscrewing. This is now getting scary when Lou has me assisting.
Now just about everyone associated with this airport has been operated on by Lou. We found a few old-timers sitting around drinking coffee saying, "Doc, just bang it harder."
By this time one of the old-timers, John the mechanic, shows up. “Doc get out of the way let me take a look … I'll be back in a minute.” We figured he went off to get his tool chest and started to look for him thinking he'd need help carrying things. |
 |
| Ryan, Brad, Lou and myself Saturday on the flight home. Notice smiles on all, we had a good time! |
John came back a few minutes later and the only thing in his hand was a bigger can of silicone spray. He gave it a squirt and said, "…put it all back together, you're good to go." We all look at him and think, we've tried this already, but we do as we are told by the consultant and, damn it, the plane starts right up.
Now you can imagine that all this is going through our master pilots mind, not to mention the hard time he is about to get from his old friend. John the mechanic says to Lou, “Don’t worry Doc I have seen this before and you just didn't know where to spray." See one, do one, teach one!
We made it down to pick up Brad about 10:30 PM, refueled, had a sandwich, and got into Tampa about midnight. Of course our car and driver were waiting at the wrong airport, but he eventually found us.
The workshop begins with an introduction by Jason Heath, Director of Marketing for Omnilife scienceTM and a presentation by. Dr. Keppler, Design Rationale for the ARCTM Tissue Sparing Hip, and one by Dr. Charles Bryant on the Anterior Approach.

Jason Heath, Director of Marketing introducing Dr. Louis Keppler


Excellent facility with great video, lecture and workshop features.
 |
|
| Dr. Maurice Jove |
Some comments by Dr. Maurice Jove
When I was invited to the workshop I was intrigued with the opportunity to be able to venture into an environment where guys in practice for many years with polished surgical skills could sit and informally discuss and observe each others desire to perform what is now called tissue sparing surgery. I have been trying for years to minimize my incisions, minimize the trauma to the gluteal musculature and reduce the post op bleeding. I had become concerned with the self advancing salesmanship of the two incisional approach as the rates of failure from this technique have climbed in numbers. The small posterior incisions still experiences a higher dislocation rate. 
My old trusty lateral incision with an anterior dislocation which allowed for an extensile exposure had worked well for many years with one primary hip dislocation in over 2500 hip arthroplasties. Now to be able to combine this with a smaller, more anatomic and intelligently designed femoral stem - that was intriguing and potentially more efficient.
 |
| The ARCTM Stem with modular trial neck. |
The opportunity to show it to others with the same goals in mind was the venue at the Tampa meeting. The cadaver lab was the avenue for education and training.
The new stem design, somewhat radical but with excellent biomechanical design, proved a simple and reproducible construct in the hands of the least skilled present. It was easy to insert with very little trauma to the surrounding muscles due to the anatomic curved design. With the use of special retractors the prosthesis is easily implantable through a small, minimally invasive incision. The surrounding tissues then easily spared from the trauma of reaming and broaching of lateralizing stems.
Visualization of the acetabulum was easily and clearly done with minimal trauma. The result, a hip with-built in stability and mobility. The way it was meant to be.
Dr. Jove’s surgical technique will be featured in our next newsletter.
Control of the Educational Process
I have had the opportunity to spend a significant amount of time in Australia and consider it a real honor to be one of the few international Affiliate Members of the Australian Orthopaedic Association (AOA). I have reported on this fine group in past newsletters and commented on my friend Dr. Bruce Shepherd’s book “Memories of an interfering man.” Once again, I find this man to be ahead of his time in many regards.
At the 2006 Annual AOA Scientific Meeting held that year in Canberra, the nations capital, there was considerable unrest within the AOA. Bruce Shepherd, John Harrison (both past AOA presidents), and Dr. Allen Turnbull were reviewing their concerns with the Royal Australasian College of Surgeons (RACS). At the Annual Business meeting Bruce presented a motion to separate the AOA from RACS. There was lively debate that reminded me of the televised British Parliament style discussions. The motion did not carry, but I just received my AOA July eNEWSLETTER Bulletin with the following lead from the President, Ian C. Dickinson.
 |
|
| Ian C. Dickinson |
On a number of occasions in its history, AOA has considered separating from the Royal Australasian College of Surgeons (RACS). In recent times, this was referred to as forming an academy, but any discussion around this issue is essentially a debate about separation, no matter how we may choose to describe this major strategic issue.
Separation from RACS would provide orthopaedic surgeons primacy in relation to orthopaedic education and standards, ultimately for the benefit of patient care.
Several recent decisions by RACS have highlighted the lack of proper consultation and consideration of the views of AOA and our members, to the potential detriment of standards of care of patients with orthopaedic conditions. As a result, the Board unanimously decided at its meeting on 26 June to spend funds on undertaking a professional cost/benefit and risk analysis of seeking direct accreditation by the Australian Medical Council (AMC) for our Surgical Education and Training program. The Board has an unambiguous intent to separate. Read more
 Unintended Results of the Gift Ban Unintended Results of the Gift Ban
Massachusetts Code of Conduct: Harm to Massachusetts Companies and Economy
As reported by Policy and Medicine www.policymed.com
The medical device industry was pleased last week when the Massachusetts House of Representatives voted 145-4 to repeal the “gift ban” law as part of a bigger piece of economic development legislation.
I encourage all to read their publication and subscribe to their service.
The paragraph below sums up this overreaction, and how it lead to the creation of laws without thinking them through.
The unintended results of the gift ban have caused a “loss of some convention business, and a reduction in medical training and clinical research.” It has also “sent out a message that has chilled opportunities for training and clinical research.” The ripple effect of this legislation has also impacted the restaurant business.
- Representative Dempsey during a House floor debate.
Final Thoughts
One of the lessons learned with life experiences is to stay involved. That is often easier said than done. I am sure we all have examples of our “don’t give up” moments.
Bruce Shepherd’s involvement, even while retired from surgery, has helped lead the AOA in standing up for its own independence and control on quality. Overreaction to the Justice Department's probe into the pharmaceutical and device industry has, in my opinion, created more problems than it has solved. Massachusetts is one of the states that has taken several legal actions that now, in hindsight, has been deemed harmful.
So please stay involved, find the time, or support those that are willing.
July 29, 2010

Surgeon Owned Distribution
We feel obligated to keep this discussion in front of all our readers. We reported on this in an editorial posted this past April.
JISRF is not an advocate of this type of activity and we encouraged caution to any surgeon considering this type of activity. Furthermore, we bring to our readers attention to a recent white paper published by Stephen J. Immelt and Ronald L. Wisor Jr. of the law firm Hogan & Hartson.
I do not intend to quote their entire paper, but I do recommend that everyone take the time to read it.
The following is their Conclusion:
Conclusion
At bottom, POIs are really about creating opportunities for physicians to profit from their
own referrals, a proposition antithetical to the fraud and abuse laws. The abuses inherent to the various POI business models are currently occurring in the markets for orthopedic and implants, presenting conflicts of interest that interfere with physician judgment about whether to perform a procedure, the best products to use and where procedures are performed. These conflicts of interest not only raise significant health and safety risks for patients, but also present significant legal risks for physicians, hospitals and implant manufacturers of being prosecuted or penalized for violating the fraud and abuse laws. Given the confluence of legal problems and ethical concerns, the questions is not whether POIs will come under government scrutiny, but when.
Stephen J. Immelt
Ronald L. Wisor Jr.

Timothy McTighe, Dr. H.S. (hc)
Executive Director
Joint Implant Surgery & Research Foundation
You will need the Adobe Reader to view and print these documents. |