Most investigators credit Branemark (1965) in Sweden with the idea of a percutaneous, osteointegrated prosthesis which has been successful in dental implantation. [1] In 1997, R. Branemark reported on the first femoral intramedullary percutaneous device using a 12 cm screw-type device for a patient with an above-knee amputation. [2] In 1999, ESKA produced the Endo-Exo Femurprosthesis (EEFP) which was first implanted into the femoral canal of a young motorcyclist who lost his leg in an accident and subsequently used for a number of patients in Germany. There have been variations in the design, including some types to allow proximal fixation to other devices such as a hip replacement, but commonly the device is a modular, noncemented device that fits within the intramedullary canal of the femur and has a hardpoint attachment that exits through the skin. [3] Three of our co-authors (JK,RK, & TC) have been to Germany, studied this procedure and reviewed historical outcomes. The original device utilized a spongiosa surface of casted cobalt chrome that allows for a porous surface for bone ingrowth.
Challenges The clinical challenges of an OI-style implant are twofold. First, the device must have a stable and secure fixation within the femur shaft for the forces to be transmitted from the subject's hip and thigh musculature to the distal prosthesis. Second, the issue of the skin implant junction must be managed to prevent infection from traveling up from the skin to the bone of the femur. Since the original device was made of cast Co-Cr our team felt a forged titanium alloy rod with a more contemporary porous coating of commercially pure (CP) titanium would provide for a better osteointegration.
The reported clinical experience has shown that the implant can be securely fixed into the medullary canal of the distal residual femur. This stable fixation is achieved by preparation of the femur with reamers and precision cutting instruments prior-to implantation.
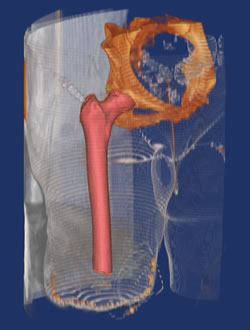
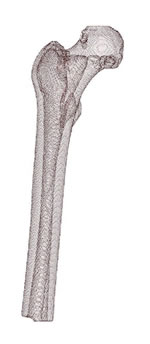
Preoperative Considerations Preoperative planning requires consideration of the local stump, including scars or burns as well as radiographic determination of the length and diameter of the prosthesis. A CT scan is helpful for determining the necessary implant size and limb length. Typically at least 12 to 15 cm of femoral shaft is needed for stable fixation. 3 D and Finite Element Modeling are done to provide for customization of the device for the individual bony parameters of the patient. Potential Benefits Benefits include the patient having a more normal gait pattern with little to no pain via the use of prosthesis for transfemoral-level amputations. In essence, this would lead to a higher quality of life, such as higher levels of independence in daily living, physical activity levels, self-care and employment opportunities that would not be possible with the continued use of a socket-style prosthesis that joins the residual stump to a prosthesis. Material and Methods Patient Profile Index patient is a 63-year-old African American Female. She is 170cm tall and weighed 75kg. Primary amputation completed 78 days prior to this procedure. Revision amputation was preformed 32 days prior-to index surgery due to wound healing problems and pain at the medial aspect of the residual limb scar. The patient is a medical professional with more than 40 years of critical care experience. She did not want to accept permanent disability and has a strong desire to return to clinical practice. She is married. A Nonsmoker. No illegal or recreational drug usage. She had no other co-morbidities. She takes no medications on a regular basis other than pain medications following the amputation. She has multiple medication allergies to include penicillins, cephalosporins, and a contact skin anaphylactic reaction to latex based products. Diagnosis Indication for amputation was a multiple recurrent low-grade chondrosarcoma of the right distal femur. The lesions did not fit the typical classification and could be described as juxtacortical. The classification of the lesion as a malignant cartilage tumor was based on it clinical behavior as well as its histology. Microscopic examination demonstrated bland appearing cartilage with minimal atypia and one mitotic figure per high-powered field of microscopic view. The patient's first surgery for this was at the age of 16. She had undergone a total of 14 prior surgeries for this issue with incomplete resection and local recurrence. Prior-to amputation the tumor was found to have extended into the popliteal fossa and was clearly encasing the neurovascular bundle. The patient was experiencing vascular claudication symptoms on ambulation prior-to the amputation.
Preoperative Counseling The patient had been counseled by experienced prosthatists on the design and function that was anticipated with a conventional suction suspension system prosthesis for the transfemoral level. She was not satisfied with the level of function this was anticipated to afford after final fitting.
The patient was counseled at length on the details of the staged Osseointegration implant system designed by a private orthopaedic device team and manufactured by Signature Orthopedics LTD, in Sydney Australia. She was shown YouTube videos of patients who had undergone similar surgery in Europe with a similar device. She preformed her own extensive literature review on the topic of osseointegration implant systems. She was consented per the IRB approved protocol. She was given a copy of the PI's financial disclosure statement prior-to completion of the consent documents. Global Effort & Collaboration A high lever of experienced orthopaedic surgeons, implant designers and device manufactures (CDD,LLC) have been collaborating on the refinement of pre-existing European technology (Eska) Orthodynamics "Intregral Leg Prosthesis (Endo-Exo). The Integral Leg Prosthesis incorporates Spongiosa Metal™ II technology for secure primary fixation and provides a 3 dimensional structure for subsequent osseointegration of the implant. Results have been very encouraging with this device, however this has not been available in the United States. So our team took on the project of designing an updated device with material (titanium alloy & CP porous coating) that was felt would provide for more precision in fabricating a custom device and a more contemporary porous structure to enhance bony fixation. Our senior author has significant training with battlefield wounds from his military experience from 1993 to 2005 including being part of the 67th Forward Surgical Team, Operation Iraqi Freedom in 2003. His Orthopaedic Oncology Fellowship at UCLA, Department of Orthopaedic Surgery in 2005 provided additional training and interest in the field of limb amputation and resection arthroplasty. Three other members of our team (JK, RK, TC) have all been to Europe and received training on the Eska Endo-Exo device. Another member (EM) has significant experience and expertise in treating joint infections. Our remaining team members (DB, TM) have significant experience in design and fabrication of orthopaedic devices. Surgeons are experts at making the most of conventional 2D image data to prepare for their surgeries. However, even the best planners can struggle with limited information that is available in 2D images and with the inability to try out multiple approaches before entering the OR. Fortunately, 3D virtual surgical planning is available to remove many of the hurdles involved in determining the best plan and transferring it to reality.
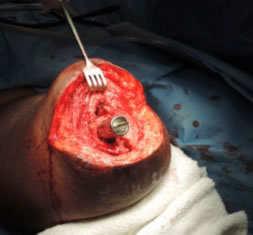
Current software is now available to aid in preparation, planning while guiding the production of your custom device, along with planning your surgery. Custom fabrication can then be on sound scientific demonstration of fit and fill of the required parameters to ensure proper fit of the device. Surgical Technique Primary amputation completed 78 days prior to this procedure. The patient's amputation was preformed with a clear surgical margin of more than 4 cm with no residual tumor was present. The amputation was carried out at the distal 1/3 of the diaphysis. The amputation was completed in the classic fish mouth style of equal anterior and posterior flaps of skin and muscle. The femur was transected 5 cm proximal to the skin incision. The closure was preformed with suture myodesis of the major muscles to the transected femur. The posterior fascia was sutured to the anterior fascia. The skin was approximated with simple surgical staples. Surgical Case
Approximately six to eight weeks after the implantation of the endoprosthesis, when the wounds are well healed, the second procedure is done to create the stoma and attach the transdermal coupler. This is usually done as an outpatient procedure. The secondary procedure will be reported on as a follow-up to this case report. We are excited that this Osteointegration implant (OI) for Transfemoral Amputation will provide an alternative treatment for patients for whom a traditional-socket-type above-the-knee prosthesis presents difficulties. References:
Related Articles:
You will need the Adobe Reader to view and print these documents. |
|


 Figure 2. Titanium forged IM Rod with a sintered CP porous coating.
Figure 2. Titanium forged IM Rod with a sintered CP porous coating.